Knee
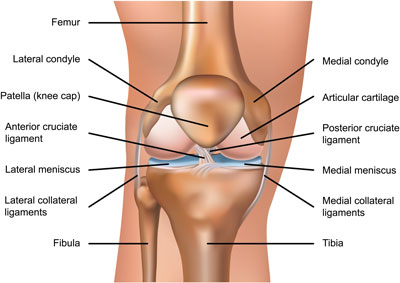
The distal end of the femur, a long bone, together with the proximal tibia and the posterior surface of the patella, a triangular bone, form the knee joint.
This joint is a hinge-type joint (not to be confused with “Hamid’s hinge” 😂), meaning the end of the femur fits into the tibial articular surface like a pulley, allowing movement primarily in one direction.
In the thigh, we have the quadriceps muscles, which continue over the patella as the patellar tendon (soft tissue) and surround the patella.
The patella forms the anterior part of this joint, and due to its position, it is highly susceptible to injury in knee trauma.
In cases where part of this bone is displaced, surgery is not required, and a splint or cast is used to stabilize the knee. Depending on the severity of the injury, no weight should be placed on the knee for six to eight weeks.
If the bone is fractured, it can be realigned using wires or pins. In some cases, the bone fragments are so small and shattered that they cannot be repositioned, and the fragments must be removed surgically (an example of a shattered knee surgery by Dr. Ali Moazzami Pour is also posted on the Instagram page, with incredible results).
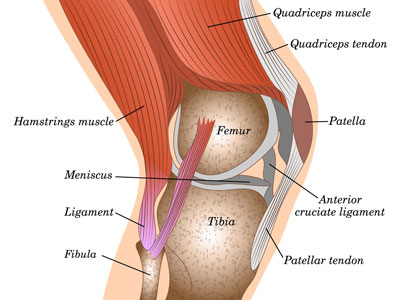
The presence of the patella in this joint prevents the knee from overextending.
Around the head of the tibia, there is a thick cartilage called the meniscus.
The medial meniscus is C-shaped and wide, while the lateral meniscus is O-shaped and smaller in size.
There is a surgical procedure called meniscectomy in this area, in which all or part of these menisci are removed.
Additionally, four ligaments are present in the knee joint:
Medial collateral ligament (MCL)
Lateral collateral ligament (LCL)
Anterior cruciate ligament (ACL)
Posterior cruciate ligament (PCL)
The anterior cruciate ligament is crucial for knee stability, and in individuals with ACL injury, knee dislocation is very common. In such cases, surgery becomes necessary.